Implementation Science
- Martin, G. P., Kocman, D. , Stephens, T. , Peden, C. J., Pearse, R. M. and , (2017), Pathways to professionalism? Quality improvement, care pathways, and the interplay of standardisation and clinical autonomy. Sociol Health Illn, 39: 1314-1329. doi:10.1111/1467-9566.12585
- Stephens, T. J., Peden, C. J., Pearse, R. M., Shaw, S. E., Abbott, T., Jones, E. L., … EPOCH trial group (2018). Improving care at scale: process evaluation of a multi-component quality improvement intervention to reduce mortality after emergency abdominal surgery (EPOCH trial). Implementation science : IS, 13(1), 142. doi:10.1186/s13012-018-0823-9
Example: Mixed Methods Evaluation
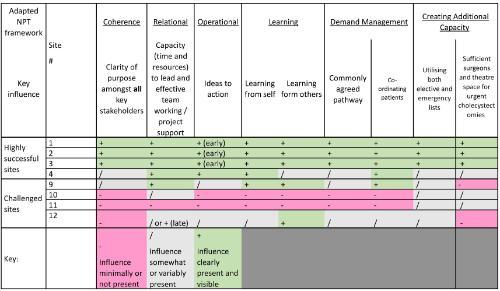
Selected figures from the mixed methods evaluation of the Royal College of Surgeons of England CholeQuIC project, which was designed to support surgeons in leading system change to reduce time to urgent laparoscopic cholecystectomy. The time-series chart demonstrates the overall reduction in variation in time to surgery that occurred in the patient cohort over time.
-page-001-500x375.jpg)
The grid shows the difference between the 4 most improved sites in the project (those that at least doubled their numbers of patients having surgery within 8 days; the project goal) and the 4 challenged sites that did not show any significant change in relation to the influences hypothesised to be most important for success during the improvement project.