Over the last 25 years our research group has been referred over 400 patients suspected to have insufficient adrenal hormone production (Familial Glucocorticoid Deficiency). This deficiency results in undetectable levels of cortisol, a hormone responsible for increasing blood sugar levels and metabolism, and elevated levels of ACTH, a hormone that regulates cortisol levels.
Through novel gene discovery techniques, mutations in many genes have been discovered to cause this insufficiency through mechanisms such as defective signalling, cholesterol transport and DNA replication. 65% of patients in our study have been diagnosed with a mutation in one of these genes and it is hoped that through advanced sequencing techniques we will discover further defective genes and be able to diagnose the remaining 40%.
For more information on the causes, symptoms and how Adrenal Insufficiency is diagnosed please visit our Patient Information page.
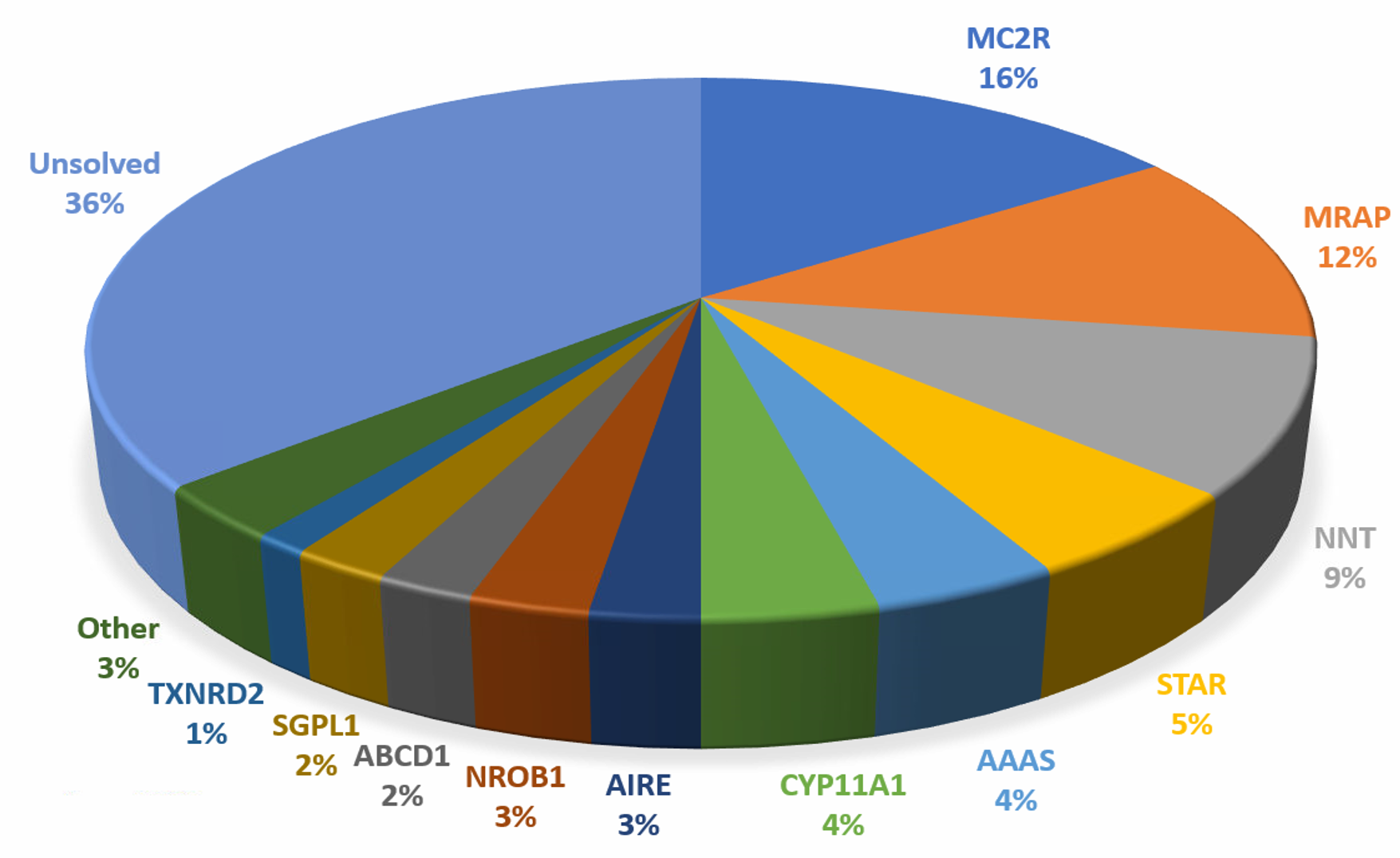
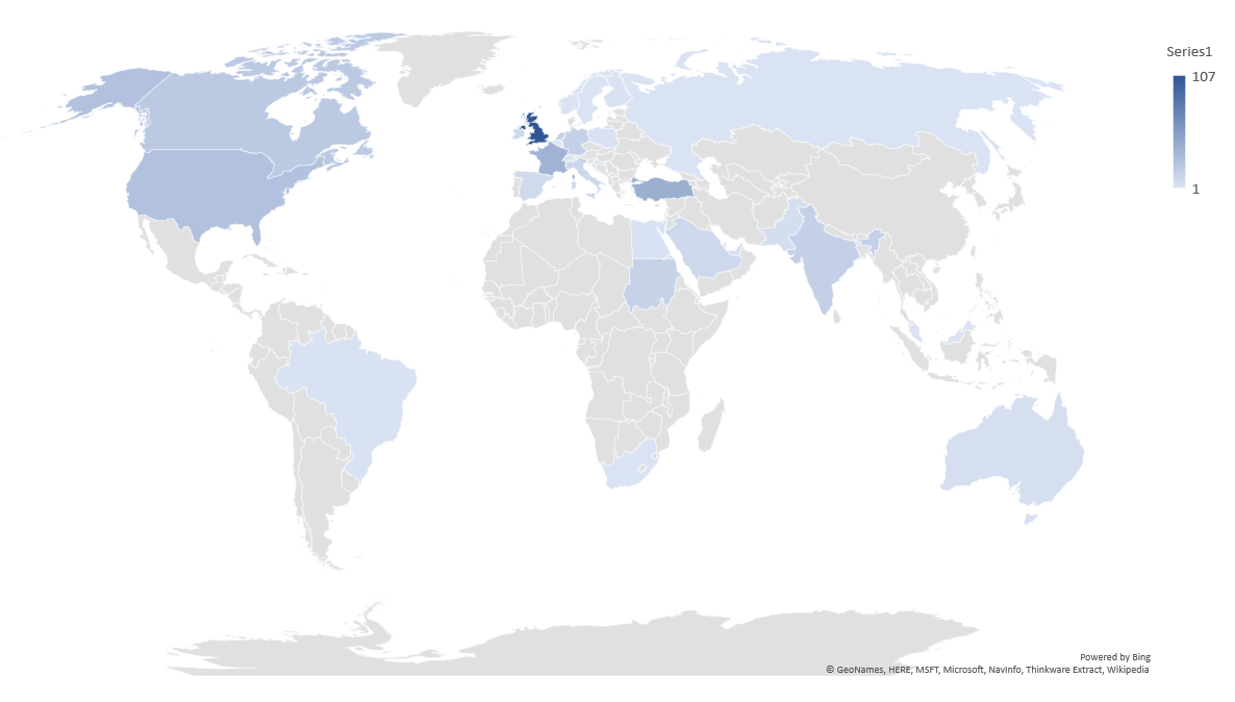
Our cohort of 400 patients with suspected FGD consists of 352 families from over 30 countries. All cases had low or undetectable serum cortisol paired with an elevated plasma ACTH level. Following the discovery of MC2R as a cause of FGD (25% of cases), 7 further genes have been identified in our cohort, MRAP (20%), NNT (8%), STAR (7%), CYP11A1 (3%), MCM4, TXNRD2 and SGPL1 (each 1%). These genes are involved in diverse pathways with phenotypes resulting from defective ACTH signalling, cholesterol transport, steroidogenesis, cellular redox homeostasis, DNA replication or sphingolipid metabolism. The finding of further gene defects be they; novel genetic aetiologies, Copy Number Variations or non-coding variation in known genes will improve the diagnosis for the 40% of our cohort yet to have a genetic diagnosis.
Furthermore, the study of these genes and the pathways they interact with builds our understanding of the phenotypes caused by certain mutations and allows for better treatment regimens for patients.
For a review of Primary Adrenal Insufficiency and its causative genes please read the following;
Maharaj A, Maudhoo A, Chan LF, Novoselova T, Prasad R, Metherell LA, Guasti L(2019). Isolated glucocorticoid deficiency: Genetic causes and animal models. Journal of Steroid Biochemistry and Molecular Biology vol. 189, 73-80.
Chan LF, Campbell DC, Novoselova TV, Clark AJ, Metherell LA. Whole-Exome Sequencing in the Differential Diagnosis of Primary Adrenal Insufficiency in Children. Front Endocrinol (Lausanne).2015 Aug5;6:113
Chung TT, Chan LF, Metherell LA, Clark AJ. Phenotypic characteristics of familial glucocorticoid deficiency (FGD) type 1 and 2. Clin Endocrinol (Oxf). 2010 May;72(5):589-94.
For selected specific genes please follow the links below;
MC2R
Clark AJ, McLoughlin L, Grossman A. Familial glucocorticoid deficiency associated with point mutation in the adrenocorticotropin receptor. Lancet. 1993 Feb 20;341(8843):461-2.
MRAP
Metherell LA, Chapple JP, Cooray S, David A, Becker C, Ruschendorf F, Naville D, Begeot M, Khoo B, Nurnberg P, Huebner A, Cheetham ME, Clark AJ. Mutations in MRAP, encoding a new interacting partner of the ACTH receptor, cause familial glucocorticoid deficiency type 2. Nat Genet. (2005) 37:166-70.
STAR
Metherell LA, Naville D, Halaby G, Begeot M, Huebner A, Nürnberg G, Nürnberg P, Green J, Tomlinson JW, Krone NP, Lin L, Racine M, Berney DM, Achermann JC, Arlt W, Clark AJL. Non-classic lipoid congenital adrenal hyperplasia masquerading as familial glucocorticoid deficiency. J Clin Endocrinol Metab. (2009) 94(10):3865-71.
CYP11A1
Maharaj A, Buonocore F, Meimaridou E, Ruiz-Babot G, Guasti L, Peng HM, Capper CP, Burgos-Tirado N et al.(2019). Predicted benign and synonymous variants in CYP11A1 cause primary adrenal insufficiency through missplicing. Journal of the Endocrine Society vol. 3, (1) 201-221.
SGPL1
Settas N, Persky R, Faucz FR, Sheanon N, Voutetakis A, Lodish M, Metherell LA, Stratakis CA(2019). SGPL1 deficiency: A rare cause of primary adrenal insufficiency. Journal of Clinical Endocrinology and Metabolism vol. 104, (5) 1484-1490.
Prasad R, Storr HL, Guasti L, Maharaj A, Meimaridou E, Hadjidemetriou I, Metherell LA, (2017). Sphingosine-1-phosphate lyase mutations cause primary adrenal insufficiency and steroid-resistant nephrotic syndrome. Journal of Clinical Investigation
NNT
Meimaridou E, Kowalczyk J, Guasti L, Hughes CR, Wagner F, Frommolt P, Nürnberg P, Mann NP et al.(2012). Mutations in NNT encoding nicotinamide nucleotide transhydrogenase cause familial glucocorticoid deficiency. Nat Genet vol. 44, (7) 740-742.
TXNRD2
Prasad R, Chan LF, Hughes CR, Kaski JP, Kowalczyk JC, Savage MO, Peters CJ, Nathwani N, Clark AJ, Storr HL, Metherell LA. Thioredoxin reductase 2 (TXNRD2) mutation associated with familial glucocorticoid deficiency (FGD). J Clin Endocrinol Metab. (2014) 99(8):E1556-63.
MCM4
Hughes CR, Guasti L, Meimaridou E, Chuang C-H, Schimenti JC, King PJ, Costigan C, Clark AJL et al.(2012). MCM4 mutation causes adrenal failure, short stature, and natural killer cell deficiency in humans. JOURNAL OF CLINICAL INVESTIGATION vol. 122, (3) 814-820.